
METABOLIC DISORDERS
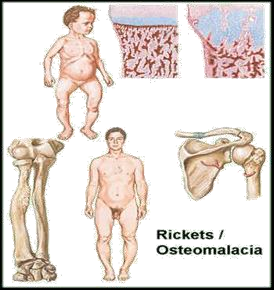
OSTEOMALACIA AND RICKETS
- Decalcification and softening of bones.
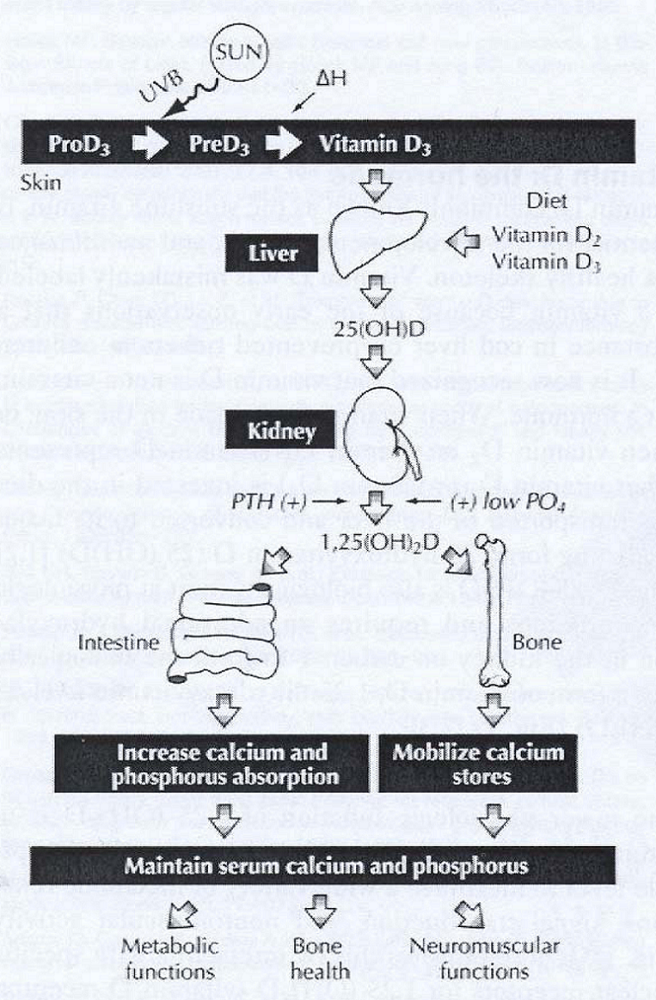
- Due to a lack of vitamin D or a problem with the body’s ability to break down and use this vitamin.
- Rickets in children.
- In adults, the condition is called osteomalacia; and in children, it’s known as rickets. Each one is a condition where prolonged and excessive vitamin D deficiency causes bones to soften, weaken, and easily fracture.
Rickets
- Disease of growing bones of children (in it epiphyseal plate not closed) in which defective mineralization occurs in both bone and cartilage of epiphyseal growth plate.
Osteomalacia
- Disorder of mature bones in adult (after epiphyseal plate closure) in which mineralization of new osteoid bone is inadequate or delayed
RISK FACTORS
- Chronic diarrhea
- GIT malabsorption
- Lack of exposure to sunlight
- Pregnancy
- Avoidance of milk
- Sedentary lifestyle
- Renal disease
- Use of strong sunscreen
CLINICAL/DIAGNOSTIC MANIFESTATION
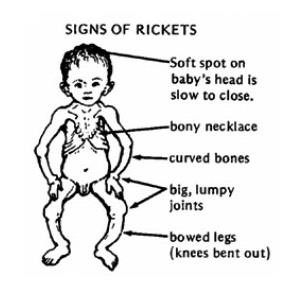 Fractures
Fractures- Persistent and diffuse skeletal pain
- Progressive deformities of bones
-
- Bowed legs
- Knock knees
- Rachitic rosary
- Enlarged wrists and ankles
- Pigeon breast
-
- Progressive muscle weakness
- Decreased serum levels of Calcium (44-107 IU/L)
- Looser zones on X-ray.
- Roentgenograms shows bone demineralization and multiple bone deformities. (white: more dense; otherwise: black)
- Elevated serum alkaline phosphatase.
NURSING INTERVENTIONS
 Assess posture and gait, note ability to walk with or without aid.
Assess posture and gait, note ability to walk with or without aid.- Note ability to walk requested distances.
- Check bony prominence for pressure sores.
- Assess shapes of bones throughout the body.
- Administer prescribed diet.
- Rich in Calcium
- Rich in Vitamin D (tuna, salmon, mackerel)
- Discuss purpose of physical therapy.
- Assist to a position of comfort.
- Administer prescribed analgesics.
- Gentle back massage.
- Instruct regarding home safety.
- Teach family the effects of Calcium and Vitamin D on the body and the factors affecting absorption.
- Teach client on the signs of fracture.
- Follow up care as needed.
Difference Between Osteoporosis & Osteomalacia
- Osteoporosis refers to the degeneration of already constructed bone, making them brittle,
- While osteomalacia is an abnormality in the building process of bone, making them soft.
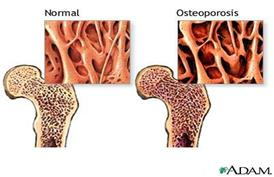
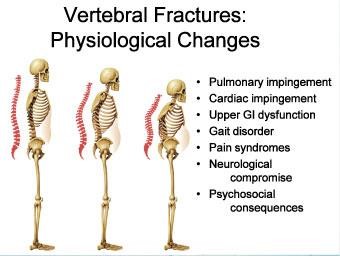
OSTEOPOROSIS
- Decrease in the bone mass and density with a change in bone structure.
- May be ASYMPTOMATIC until the bones become fragile and a minor injury or movement causes a fracture.
- A disease of the bone characterized by a decrease in the bone mass and density with a change in bone structure
- METABOLIC BONE DISORDERS
- Osteoporosis is a metabolic bone disease that involves an imbalance between new bone formation and bone resorption.
Primary osteoporosis is the most common type; occurs most often in women after menopause because low levels of estrogen are associated with an increase in bone resorption.
Bone loss occurs predominantly in the vertebral bodies of the spine, the femoral neck in the hip, and the distal radius of the arm. Bone mass declines, leaving the bones brittle and weak.
PATHOPHYSIOLOGY
- Normal homeostatic bone turnover is altered rate of bone RESORPTION is greater than bone FORMATION reduction in total bone mass reduction in bone mineral density prone to FRACTURE.
Low bone mass/
impaired bone quality
Inadequate peak bone mass
Early menopausal bone loss
Decrease in bone mass/bone quality

Calcium/
vitamin D deficiency
Other factors
Fractures
TYPES:
Primary
-
- advanced age
- post-menopausal
Secondary
-
- Steroids use
- will inhibit formation of bones
- decrease absorption of Calcium
- increase urine Calcium loss
 Alcohol overuse
Alcohol overuse- Renal failure
- Steroids use
RISK FACTORS
- Sedentary lifestyle
- Age
- Diet: caffeine, alcohol, low Calcium and Vitamin D
- Post-menopausal
 Genetics : Caucasian and Asian
Genetics : Caucasian and Asian- Immobility
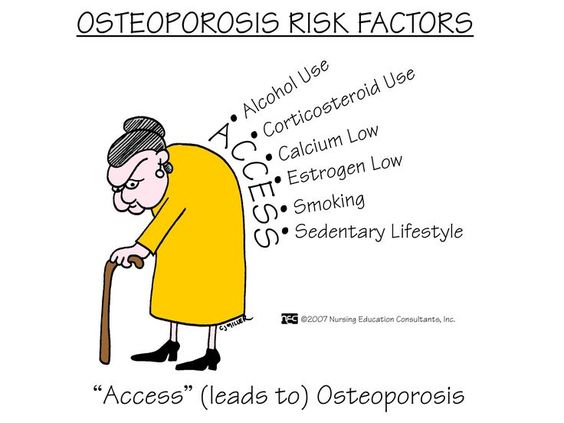
“FAST ACCESS”
- Family history of osteoporosis
- Age
- Surgical menopause following hysterectomy with or without oophorectomy
- Thyrotoxicity
- Alcohol
- Corticosteroids
- Calcium deficiancy (low intake)
- Eostrogen deficiency
- Smoking
- Sedentary Lifestyle
ASSESSMENT FINDINGS
- Low stature (stooping)
- Fracture (usually long bones)
- Bone pain
LABORATORY FINDINGS
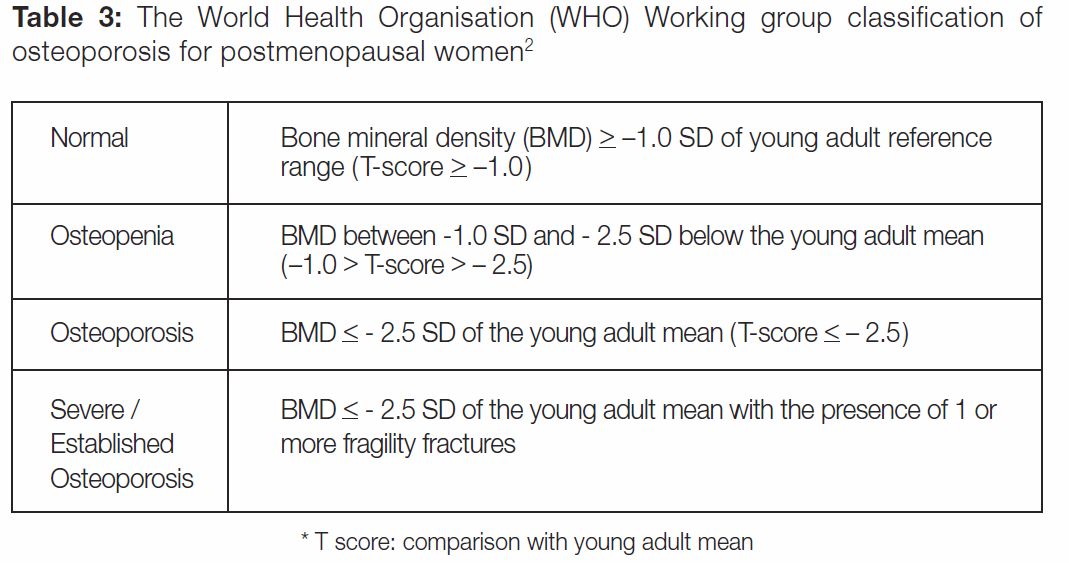
- DEXA-scan
- Provides information about bone mineral density
T-score is at least 2.5 SD below the young adult mean value
- X-ray studies
MEDICAL MANAGEMENT
- Diet therapy with Calcium and Vitamin D.
- Hormone replacement therapy.
- Moderate weight bearing exercise.
- Management of fractures.
- Medications.
-
- Calcium supplements: daily intake of calcium should be approximately 1000 mg for men and 1500 mg for postmenopausal women.
- Vitamin D supplements (800 to 1000 IU recommended daily for postmenopausal women and older adults) to enhance utilization of calcium; spending 20 minutes daily in the sun will provide adequate vitamin D.
-
- Surgical
- Kyphoplasty
- Balloon creates a cavity in vertebral body in which to inject cement
- Restores vertebral body height in 70%
- Reduces fracture
- Partially corrects kyphosis
- Vertebroplasty
- Fluoroscopic procedure where cement is injected into vertebral body
- Prevents further collapse, does not restore height
- Pain relief within 48 hours generally, effective in 75-90%
NURSING INTERVENTIONS
- Promote understanding of osteoporosis and the treatment regimen.
- Provide adequate dietary supplement of Calcium and Vitamin D.
- Instruct to employ a regular program of moderate exercises and physical activity.
- Manage the constipating side effect of Calcium supplements.
- Take Calcium supplements with meals.
- Avoid alcohol and coffee if under Calcium Therapy.
- Instruct on intake of hormonal replacement.
- Other medications:
- Selective Estrogen Receptor Modulators [SERMs] (Evista)
- Drugs that block the naturally circulating estrogen in breast tissues and other estrogensensitive tissues in the body.
Alendrolate sodium
- A synthetic drug analog of pyrophosphate that acts primarily on bone to inhibit its resorption and is used to treat and prevent osteoporosis in postmenopausal women.
- Used together with vitamin D.
Calcitonin
- Relieve pain.
- Suggest that knee flexion will cause relaxation of back muscles.
- Heat application may provide comfort.
- Encourage good posture and body mechanics.
- Instruct to avoid twisting and heavy lifting.
- Improve bowel elimination.
- Constipation is a problem of Calcium supplements and immobility.
- Advise intake of high fiber diet and increase fluids.
- Prevent injury.
- Instruct to use isometric exercise to strengthen the trunk muscles.
- Avoid sudden bending strenuous lifting.
 Provide a safe environment.
Provide a safe environment.
INFLAMMATORY CONDITIONS
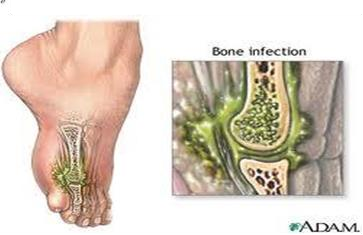
OSTEOMYELITIS
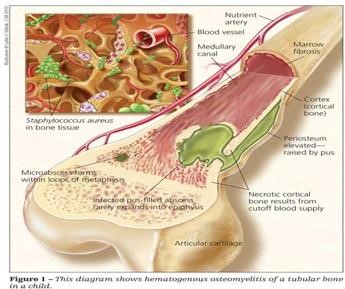 Infection of the bone and the bone marrow.
Infection of the bone and the bone marrow.- Caused by direct invasion from an open wound or a systemic infection.
- Caused by lowered body resistance and decreased blood flow to the bones
- Osteomyelitis is an infection of the bone, bone marrow, and surrounding soft tissue.
- The most common causative organism is Staphylococcus aureus.
- Inflammatory response occurs initially, with increased vascularization and edema.
ETIOLOGIES
- Escherichia coli
- Neisseria gonorrhea
- Salmonella typhi
- Staphylococcus aureus (most common)
CLINICAL & DIAGNOSTIC FINDINGS
- Fever (systemic and local)
- Pain and lack of desire to use affected limb
- Culture of drainage revealing infectious microorganism
- Elevated WBC and neutrophils (WBC: 5000-10000/mm3; Neutrophils: 50-70 %)
- Weakness, headache, nausea and vomiting
- Redness, edema and inflammation
- History of trauma
DIAGNOSTIC STUDIES
- CBC- WBC may be elevated (indicates presence of active infection).
- ESR (erythrocyte sedimentation rate) – may be elevated (indicates inflammatory process).
- Bone Scan (indicates infected bone).
- Bone lesion biopsy or culture (may reveal the causative organism).
NURSING INTERVENTIONS
- Assess site of inflammation.
- Assess drainage from irrigating tube.
- Assist in positioning to comfort.
- Maintain bed rest.
- Assist in obtaining blood specimen for culture.
- Administer antibiotics and pain medications.
- Offer fluids and monitor fluid status.
- Provide divertional activities.
TREATMENT
- Intensive intravenous (IV) antibiotics; oral antibiotic therapy for 6 to 8 weeks.
- Immobilization of affected area.
- Surgical debridement may be necessary.
 Hyperbaric oxygen therapy to stimulate circulation and healing.
Hyperbaric oxygen therapy to stimulate circulation and healing.
TEACHINGS
- Teach self-care.
- Wound care.
- Self-administration of antibiotics analgesics.
- Use of ambulatory aids.
- Complete continuity of care.
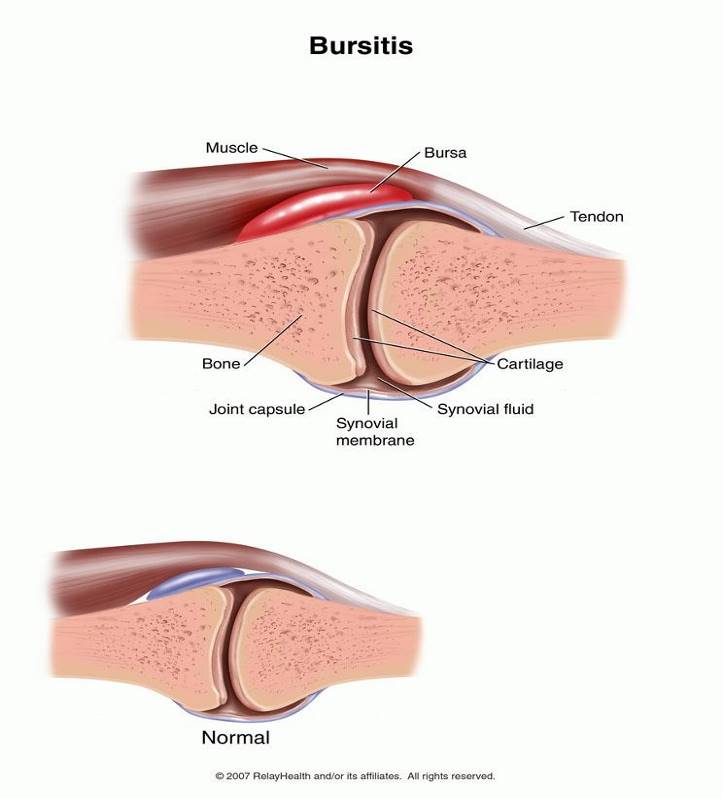
BURSITIS
– Inflammation of the bursa.
ETIOLOGIES
- Excessive trauma
- Excessive friction
- Rheumatoid arthritis
MANIFESTATIONS
- Point tenderness
- Limited ROM
- Calcified bursa
- History of repeated trauma
NURSING INTERVENTIONS
- Assess bursal area and surrounding tissues for ROM limitations.
- Apply moist compress to the area.
-
- warm: decrease swelling
- cold: prevent swelling
-
- Support inflamed tissues.
- Arm support/sling if shoulder bursa is affected.
- Administer prescribed medications.
- Arrange follow up visits.
- Refer to physical therapist for exercise regimen.
JOINT DISORDERS
Definition of Arthritis
The word “arthritis” is derived from two Greek words: arthron, meaning a joint, and – itis, meaning inflammation. Inflammation typically involves redness, heat, swelling and tenderness. So, arthritis means an inflammation joint.
Types of Arthritis
Arthritis is not a single disease with a single cause. There are dozens of different types of arthritis, each with its own cause. These are five types of arthritis which often occurs:
GOUT
TOPHI
|
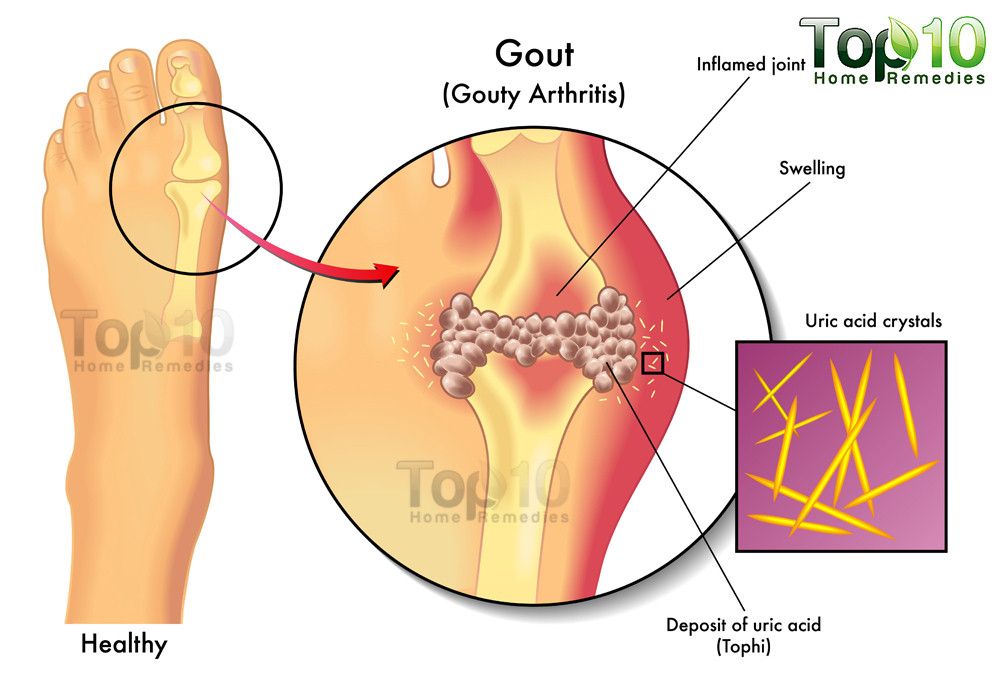
GOUT/GOUTY ARTHRITIS
- Gout is an arthritic condition resulting from a defect in the metabolism of uric acid (hyperuricemia).
- Uric acid is the end product of purine metabolism.
- Hyperuricemia may also occur in individuals receiving chemotherapy (secondary gout).
- Deposition of urate crystals in the joint spaces.
- Build up is caused by lack of enzymes to complete purine metabolism. – Common in males.
Also Known As
- Disease Of Kings
- ‘Disease of kings’ on the rise as more people get gout because of increase in obesity. Soaring numbers of patients are being admitted to hospital with gout triggered by obesity and heavy drinking. The painful illness is known as the disease of kings as it afflicted a number of monarchs including Henry VIII.
Incidence
- Primary gout has 85% incidence of all cases, of which 95% are men
ETIOLOGIES
- Buildup of uric acid crystals due to incomplete metabolism of purine.
- Increased production of uric acid secondary to increased cell destruction.
Pathophysiology
- In the body, uric acid is made by enzymatic breakdown of tissue and dietary purines. Huperuricemia develops because of underexcretion or overproduction of uric acid. In addition to accumulation in the blood, uric acid is concentrated in the synovial fluid, myocardium, kidneys, and ears. When uric acid levels reach a certain level, they crystallize, and the crystals (trophy) are deposited in connective tissue. Because the crystals are deposited in connective tissue, gout is classified as a form of arthritis.
CLINICAL MANIFESTATION
- Appearance of tophi.
- Arthritic joint deformities.
- Pain on the large toe on other joints.
 DIAGNOSTIC FINDING
DIAGNOSTIC FINDING
- Elevated serum uric acid.
- Joint tenderness.
- Red hot swollen joint.
- Joint fluid analysis shows characteristic of urate crystals.
NURSING INTERVENTIONS
- Assess severity and duration of pain.
- Place on bed rest; keep covers off the inflamed joint.
- Ice bag on inflamed joints.
- Avoid ASA (Aspirin) because it will increase uric acid.
- Administer prescribed medications.
- Example:
- Uricosuricagents :↑ urinal excretion of uric acids.
- Probenecid
- Sulfinpyrazone
- Allopurinol: inhibit/prevent uric acid formation.
- Monitor side effects of medications.
- Teach client and family to control gout through diet therapy.
- Increase fluid intake (prevent formation of renal stones).
PURINE CONTAINING FOOD
| A. HIGH (150-1000mg/100mg) | B. MODERATE (50-150 mg/100mg) |
| sardines liver and kidney sweet bread mussels meat soups brain and heart |
chicken crab and salmon bacon and pork beef and ham whole grain rice beans and spinach asparagus cauliflower |
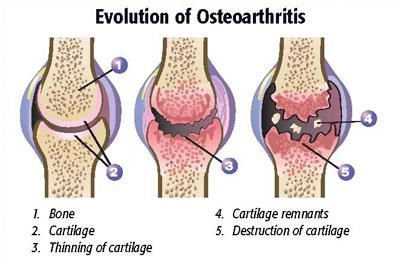
OSTEOARTHRITIS
- Osteoarthritis is a progressive, non-inflammatory disease that causes a progressive degeneration of synovial joints.
- Primarily associated with aging; may also be caused by musculoskeletal injury or conditions that cause repetitive damage to joints.
- The cartilage at the ends of the long bones and in the intervertebral joints of the spine deteriorates and leaves the ends of the bones or vertebrae rubbing together; this produces a painful, swollen joint or spine.
 Most common form of degenerative joint disorder.
Most common form of degenerative joint disorder.- Chronic, NON-systemic disorder of joints.
RISK FACTORS
- Increased age
- Obesity
- Repetitive use of joints with previous joint damage
- Anatomical deformity
- Genetic susceptibility
ASSESSMENT FINDINGS
- Joint pain
- caused by:
- commonly occurs inflamed cartilage and synovium
- stretching of the joint capsule
- irritating of nerve endings
- Stiffness
- commonly occurs in the morning after awakening
- last only for less than 30 minutes
- decreases with movement, but worsens after increased weight bearing activity d. crepitation may be elicited
DIAGNOSTIC FINDINGS
- X-ray
- narrowing joint space
- loss of cartilage
- osteophytes (spurs)
- MANAGEMENT
- Weight reduction
- Occupational and physical therapy
- Pharmacologic management
- Use of NSAIDS
- Topical analgesics
- Intra-articular steroids to decrease inflammation
- NURSING INTERVENTIONS
- Provide relief of pain.
- Administer prescribed analgesics.
- Application of heat modalities. ICE packs maybe used in the early acute stage.
- Plan daily activities when pain is less severe. Pain medications before exercising.
- Advise patient to reduce weight.
- Aerobic exercises
- Walking
- Administer medications.
- NSAIDS
- Mefenamic Acid
- Ibuprofen
- Naproxen
- Endometacin
- NSAIDS
- Position the client to prevent flexion deformity.
- Use of foot board, splints and pillows.
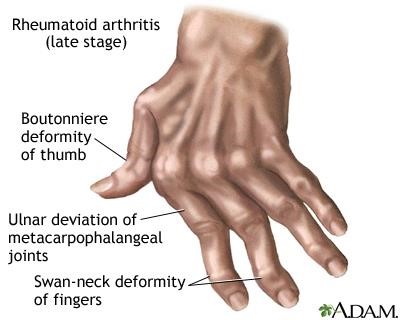
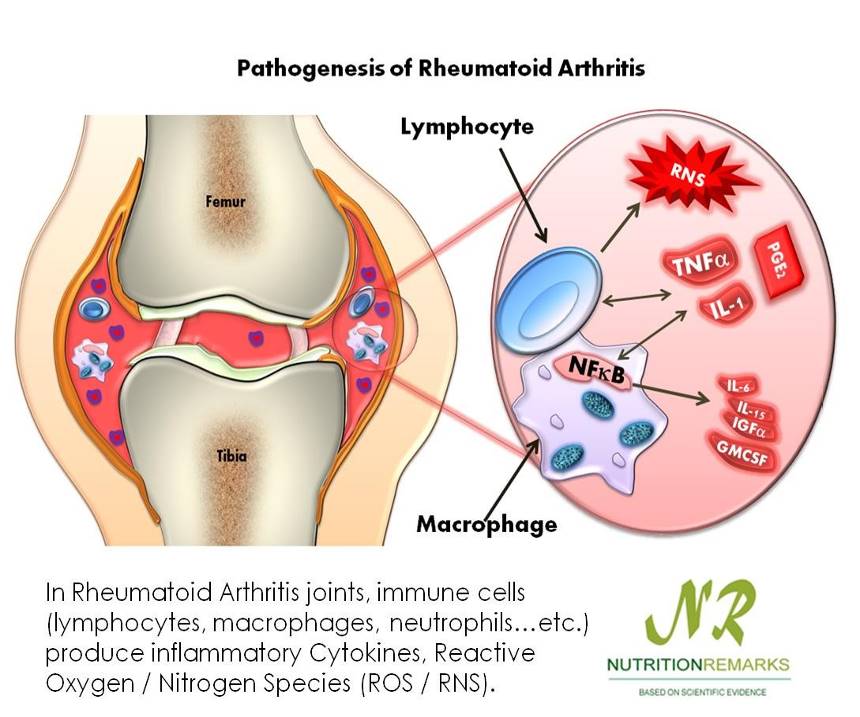
RHEUMATOID ARTHRITIS
- Rheumatoid arthritis is a chronic, systemic autoimmune disease that affects all areas of the body; inflammatory responses occur in all connective tissue. Early symptoms include inflammation of the synovial joints.
- Joint involvement progresses in stages; if disease is diagnosed early, permanent joint deterioration may be prevented.
 The synovium becomes thickened and inflamed, and fluid accumulates in the joint space; this causes a pannus to form.
The synovium becomes thickened and inflamed, and fluid accumulates in the joint space; this causes a pannus to form.- The pannus tissue erodes the cartilage and destroys the joint.
- In medicine, pannus is any abnormal tissue that: Contains blood vessels.
- Type of chronic systemic inflammatory arthritis and connective tissue disorder affecting more women (ages 35-45) than men—3:1.
FACTORS
- Genetic
- Autoimmune connective tissue disorders
- Fatigue, emotional stress, cold, infection
ASSESSMENT FINDINGS
- Joint involvement is symmetrical and bilateral.
- Characteristically beginning in the hands, wrist and feet.
- Joint stiffness occurs early morning, lasts more than 30 minutes, not relieved by movement, and diminishes as the day progresses.
- Joints are swollen and warm.
 Painful when moved.
Painful when moved.- Deformities are common in the hands and feet causing misalignment.
- Rheumatoid nodules may be found in the subcutaneous tissues.
DIAGNOSTIC TESTS
- X-ray shows a marked deformity.
- Blood studies reveal (+) elevated ESR and CRP. ***also ANA and RF
- Arthrocentesis shows synovial fluid that is cloudy, milky or dark yellow containing numerous WBC and inflammatory proteins.
MEDICAL MANAGEMENT
- Therapeutic dose of NSAIDS and Aspirin to reduce inflammation.
- Chemotherapy with methotrexate and gold therapy.
- IM or oral preparation
- Takes several months (3-6) before effects can be seen.
- May cause bone marrow depression.
NURSING MANAGEMENT
- Relieve pain and discomfort.
- Use splints to immobilize the affected extremity during acute stage of the disease and inflammation to reduce deformity.
- Suggest application of COLD PACKS during the acute phase of pain, and then HEAT application as the inflammation subsides.
- Decrease patient’s fatigue.
- Scheduled activity when pain is less severe.
- Provide adequate periods of rests.
- Promote restorative sleep.
- Increase patient mobility.
- Advise proper posture and body mechanics.
- Support joint in functional position.
- Advise active ROM.
- Provide diet therapy.
- Patients experience anorexia, nausea and weight loss
- Gluten free diet
- Oats, wheat, cucumber
- Supplements of vitamins, iron and protein
| Definition | Gouty Arthritis | Rheumatoid Arthritis | Osteoarthritis |
| Definition | Uric acid build up in blood and causes joint swelling and pain | Inflammation of joints and surrounding tissue | Due to aging, wear and tear on a joint |
| Population | Male | Female | Both |
| Etiology | Metabolic | Autoimmune | Degenerative |
| Affected | Lower extremities | Upper extremities | Weight bearing joints |
| Hallmark Sign | Tophi | Mirror Image Ankylosis | Heberden’s Nodes
Bouchards Crepitus |
- Heberden’s nodes are hard or bony swellings that can develop in the distal interphalangeal joints (DIP) (the joints closest to the end of the fingers and toes). They are a sign of osteoarthritis and are caused by formation of osteophytes (calcific spurs) of the articular (joint) cartilage in response to repeated trauma at the joint.
- Bouchard’s nodes are hard, bony outgrowths or gelatinous cysts on the proximal interphalangeal joints (the middle joints of fingers or toes.) They are seen in osteoarthritis, where they are caused by formation of calcific spurs of the articular (joint) cartilage.
- Crepitus (also termed crepitation) is a medical term to describe the grating, crackling or popping sounds and sensations experienced under the skin and joints or a crackling sensation due to the presence of air in the subcutaneous tissue.
FRACTURE
1. A fracture is a break in the continuity of the bone.
2. Common fracture sites:
- Clavicle
- Humerus – In subpracondylar fractures, which occur when child falls backward on hands with elbows straight, there is a high incidence of neurovascular complications
 due to the anatomic relationship of the brachial artery and nerves to the fracture site.
due to the anatomic relationship of the brachial artery and nerves to the fracture site. - Radius and ulna
- Femur (often associated with child abuse)
- Epiphyseal plates (potential for growth deformity)
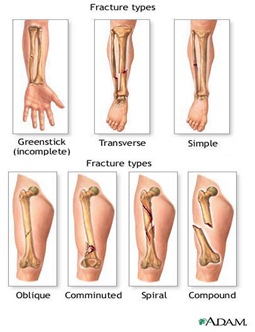
3. Types of Fracture
- Closed or simple fracture – The bone is broken, but the skin is not lacerated.
- Open or compound fracture – The skin may be pierced by the bone or by a blow that breaks the skin at the time of the fracture. The bone may or may not be visible in the wound.
- Transverse fracture – The fracture is at right angles to the long axis of the bone.
- Greenstick fracture – Fracture on one side of the bone, causing a bend on the other side of the bone.
- Comminuted fracture – A fracture that results in three or more bone fragments.
- Oblique Fracture – The fracture is diagonal to a bone’s long axis.
- Spiral Fracture – At least one part of the bone has been twisted.
4. Complications of fractures include:
- problems associated with immobility (muscle atrophy, joint contracture, pressure sores)
- growth problems ( in children)
- infection
- shock
- venous stasis and thromboembolism
- pulmonary emboli and fat emboli
- and bone union problems
B. Etiology
- Fractures in children usually are the result of trauma from motor vehicle accidents, falls or child abuse.
- Because of the resilience of the soft tissue of children, fractures occur more often than soft tissue injuries.
C. Pathopysiology
- Fractures occur when the resistance of bone against the stress being exerted yields to the stress force.
- Fractures most commonly seen in children:
- Bend Fracture – is characterized by the bone bending to the breaking point and not straightening without intervention.
 Buckle fracture – results from compression failure of the bone, with the bone telescoping on itself.
Buckle fracture – results from compression failure of the bone, with the bone telescoping on itself.- Greenstick fracture – is an incomplete fracture.
- D. Assessment Findings
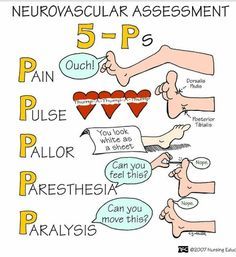
- 1. Clinical Manifestations
- The five “Ps” – pain, pulse, pallor, paresthesia, and paralysis are seen with all types of fractures.
- Other characteristic findings include deformity, swelling, bruising, muscle spasms, tenderness, pain, impaired sensation, loss of function, abnormality, crepitus, shock or refusal to walk (in small children).
 Laboratory and diagnostic findings
Laboratory and diagnostic findings- Radiographic examination reveals initial injury and subsequent healing progress. A comparison film of an opposite, unaffected extremity is often used to look for subtle changes in the affected extremity.
- Blood studies reveal bleeding (decreased hemoglobin and hematocrit) and muscle damage (elevated aspartate transaminase (AST) and lactic dehygrogenase (LHD).
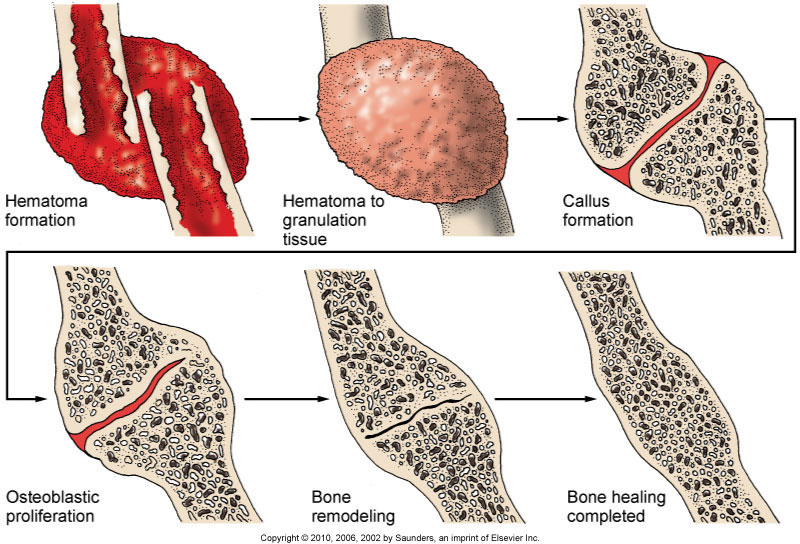
- Fracture Healing
- Reparative process of self-healing (union) occurs in the following stages:
- Fracture hematoma (d/t bleeding, edema)
- Granulation tissue → osteoid (3 – 14 days post injury)
- Callus formation (minerals deposited in osteoid)
- Ossification (3 wks – 6 mos)
- Consolidation (distance between fragments decreases → closes).
- Remodeling (union completed; remodels to original shape, strength)
- COMPLICATIONS OF FRACTURES
- Shock
- With severe injuries or femur fracture
- Neurogenic
- Hypovolemic
- Due to loss of blood volume
- Nursing Action: Replace BV, Relieve Pain, Adequate splinting/mobilization
- With severe injuries or femur fracture
- Fat Embolism Syndrome
- Occurs within 24-72 hours and can also occur up to 1 week after injury
- Seen more severe injuries
- Mostly men 20-30 y/o
- FIRST Symptom: Change in Mental status (mild agitation – Confusion – Delirium – Coma)
- Tachycardia, SOB, Dyspnea, tachypnea, petechia on shoulder and conjunctiva
- First give increased concentration of O2
- Steroids
- Occurs within 24-72 hours and can also occur up to 1 week after injury
- Compartment Syndrome
- Swelling peaks at 24-48 hours after fracture
- Signs and Symptoms
- Deep Throbbing pain that doesn’t respond to morphine
- Muscle is hard
- Diminished capillary refill
- Cyanotic nail beds
- Paralysis
- Parasthsia
- Edema – Can’t get a pulse
- Other Complications
- Thromboembolism
- Infection
- DIC – Disseminated Intravascular Coagulation
- Delayed Complications
- Delayed Union
- Healing not at rate expected possible due to Steroids, diabetic, age
- Non Union
- Bone didn’t unite the way is should
- Avascular Necrosis
- Complete blood loss to bone or neck of femur
- Reaction to Internal Fixation Devices
- Left in permanently – a rare occurrence
- Treatment is by removal of hardware
- Osteomyelitis
- Infection of bone occur with our without surgery
- Delayed Union
- Emergency: Maintain airway, assess distal pulses
E. Nursing Management
- Provide emergency management when situation warrants, for a new fracture.
- Assess the five “Ps”.
- Determine the mechanism of injury.
- Immobilize the part. Move injured parts as little as possible.
- Cover any open wounds with a sterile, or clean dressing.
- Reassess the five “Ps”.
- Apply traction if circulatory compromise is present.
- Elevate the injured limb, if possible.
- Apply cold to the injured area.
- Call emergency medical services.
- Assess for circulatory impairment (cyanosis, coldness, mottling, decreased peripheral pulses, positive blanch sign, edema not relieved by elevation, pain or cramping).
- Assess for neurologic impairment (lack of sensation or movement, pain, or tenderness, or numbness and tingling).
- Administer analgesic medications.
- Explain fracture management to the child and family. Depending on the type of break and its location, repair (by realignment or reduction) may be made by closed or open reduction followed by immobilization with a splint, traction or a cast.
- Maintain skin integrity and prevent breakdown. Institute appropriate measures for cast and appliance care.
- Prevent Complications
- Prevent circulatory impairment by assessing pulses, color and temperature, and by reporting changes immediately.
- Prevent nerve compression syndromes by testing sensation and motor function, including subjective symptoms of pain, muscular weakness, burning sensation, limited ROM, and altered sensation. Correct alignment to alleviate pressure if appropriate, and notify the health care provider.
- Prevent compartment syndrome by assessing for muscle weakness and pain out of proportion to injury. Early detection is critical to prevent tissue damage.
- Causes of compartment syndrome include tight dressings or casts, hemorrhage, trauma, burns and surgery.
- Treatment entails pressure relief, which sometimes require performing a fasciotomy.
- Prevent infection, including osteomyelitits, bys using infection control measures.
- Prevent renal calculi by encouraging fluids, monitoring I&O, and mobilizing the child as much as possible.
- Prevent pulmonary emboli by carefully monitoring adolescents and children with multiple fractures. Emboli generally occur within the first 24 hours.
GANGRENE
- The word “gangrene” comes from the Greek “ganggraina” denoting “an eating sore that ends in mortification”.
- The death of body tissue due to the loss of blood supply to that tissue, sometimes permitting bacteria to invade it and accelerate its decay.
- Gangrene is a complication of necrosis “cell death” characterized by the decay of body tissues, which become black and appearing “rotten”.
- It is caused by infection or ischemia, such as a thrombosis.
GANGRENE… WHAT IS IT???
- It is usually the result of critically insufficient blood supply.
- Often associated with diabetes and long-term smoking.
- Condition is most common in the lower extremities.
- Basically Your Blood Supply Gets Cut Off And Your Tissue Decides To Die
TYPES OF GANGRENE
- DRY GANGRENE
- WET GANGRENE
- GAS GANGRENE
DRY GANGRENE
- The early signs are a dull ache and sensation of coldness in the affected are.
- If caught early, the process can sometimes be reversed by vascular surgery.

 If necrosis sets in, the affected tissue must be removed and treated like a case of wet gangrene.
If necrosis sets in, the affected tissue must be removed and treated like a case of wet gangrene.

WET GANGRENE
- Wet gangrene occurs in naturally moist tissue and organs such as the mouth, bowel, lungs, cervix, and vulva.
- Bedsores occurring on body parts such as the sacrum, buttocks and heels (not in “moist” areas) are also categorized as wet gangrene infections.
- In wet gangrene, the tissue is infected by microorganisms, which cause tissue to swell and emit a fawol order.
- Wet gangrene usually develops rapidly due to blockage of venous and/or arterial blood flow.
- The affected part is saturated with stagnant blood which promotes the rapid growth of bacteria.
- The toxic products formed by bacteria are absorbed causing systemic manifestation of bacteria and finally death.
- The affected part is soft, putrid, rotten and dark.
- The darkness in wet gangrene occurs due to the same mechanism as in dry gangrene.



GAS GANGRENE
- Gas gangrene is a bacterial infection that produces gas within tissues.
- It is a deadly form of gangrene usually caused by bacteria.
- Infection spreads rapidly as the gases produced by bacteria expand and effect healthy tissue.
- Gas gangrene is caused by environmental bacteria.
- These Bacteria are mostly found in soil.
- These environmental bacteria enter the muscle through a wound and cause necrotic tissue and powerful toxins.
- These toxins destroy nearby tissue, generating gas at the same time.
- Gas gangrene can cause necrosis, gas production, and sepsis.
- Progression to toxemia and shock is often very rapid.


 Because of its ability to quickly spread to surrounding tissues, gas gangrene should be treated as a medical emergency.
Because of its ability to quickly spread to surrounding tissues, gas gangrene should be treated as a medical emergency.- SPECIFIC GANGRENES
- Noma is a gangrene of the face.
- Necrotizing fasciitis affects the deeper layers of the skin.
- Fournier gangrene usually affects the male genitals.
- NOMA
- Is a gangrenous disease leading to tissue destruction of the face, especially the mouth and cheek.


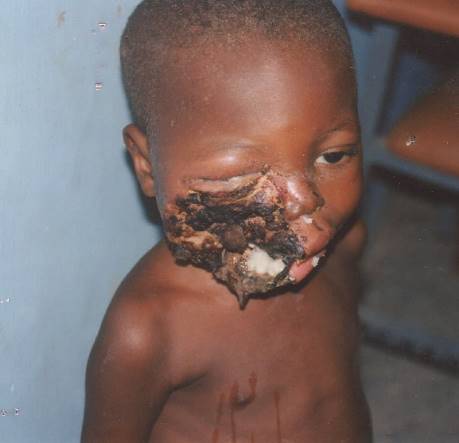 Risk factors include severe protein mal nutrition and unsanitary conditions.
Risk factors include severe protein mal nutrition and unsanitary conditions.
- NECROTIZING FASCIITIS
- Commonly known as flesh-eating disease or flesh-eating bacteria.
- Rare infection of the deeper layers of skin and easily spread within the subcutaneous tissue
 FOURNIER GANGRENE
FOURNIER GANGRENE- A type of necrotizing infection usually affecting the male genitals.
- In the majority of cases it is a mixed infection caused by both aerobic and anaerobic bacteria
- Prevention
- Cleaning the wound
- Avoid the contaminated material
- Improve circulation in patients with poor circulation
- Antitoxin
- Treatment
- Removal of the Tissue.
- In case of moist gangrene we can make scarification of Tissue. with knife or puncture the gangrenous Tissue.
- to permit the escape of toxic liquid and allowing the introduction of antiseptic inside the lesion
- Application of counter-irritant at the periphery of the affected part
- This will cause increasing of hyperemia and phagocytosis near the affected Tissue.
- Which accelerate the separation of the moist or dry gangrene from the health Tissue.
- The best treatment of gangrene is amputation of the part from the body
- High doses of antibiotic : Penicillin
- The dead tissue is removed or limbs are amputated
- No vaccine
- 10 megaunits of benzyl penicillin daily for 5 days as four 6 hourly doses Or Tetracycline 0.5 g intravenously or 1 g orally every 6 hours.
- Clostridia not sensitive to metronidazole, some other anaerobic bacteria are, so give it.
| Features | Dry Gangrene | Wet Gangrene |
| SITE | Commonly limbs | More common in bowel |
| MECHANISM | Arterial occlusion | More commonly venous obstruction |
| MACROSCOPY | Organ dry, shrunken and black | Part moist, soft, swollen, rotten and dark |
| PUTRFACTION | Limited due to very little blood supply | Marked due to stuffing of organ with blood |
| LINE OF DEMARCATION | Present at the junction between healthy and gangrenous part | No clear cut line of demarcation |
| BACTERIA | Bacteria fail to survive | Numerous present |
| PROGNOSIS | Generally better due to little septicemia | Generally poor due to profound toxemia |
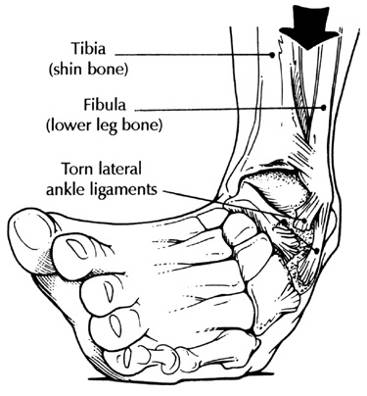 SPRAIN
SPRAIN
- A Sprain is a torn ligament. The area around the affected joint becomes Swollen, and painful. Sprains occur most in the ankles, wrist, fingers and knees.
- Sign and Symptoms of Sprain
- Pain in the joint
- Redness and swelling
- Restricted or no movement due to pain
- Discoloration (Contusion)
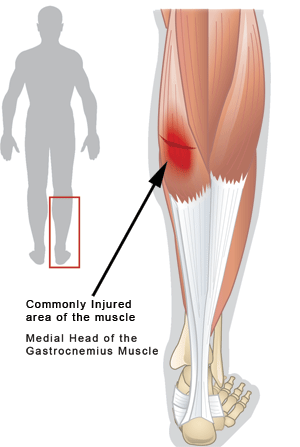
STRAIN
- A Strain is an overstretching or tear of muscle
- Sign and Symptoms of Strain
- Pain in the joint
- Redness and swelling
- Restricted or no movement due to pain
- Management of Sprain & Strain [ R.I.C.E]
- Rest
 Steady and Support the Injured part in an comfortable position
Steady and Support the Injured part in an comfortable position
- Ice
- Place Ice pack over a cloth on the injured part for about 10-20 minutes to reduce swelling and ease pain
- Do not place Ice directly on the Skin
- Compression
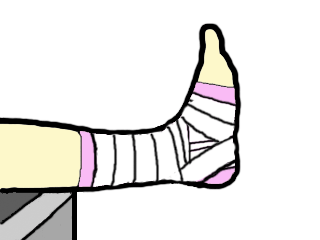 Use a Crepe Bandage to apply pressure over the Injured part
Use a Crepe Bandage to apply pressure over the Injured part
- Elevation
- Raise and support the Injured area to reduce swelling
- Seek further medical assistance if necessary
DISLOCATION
- Is a complete loss of congruity between the articulating surfaces of a joint. The bones taking part in the articulation are displaced relative to one another.
Subluxation
- In a subluxation the articulating surfaces of a joint are no longer congruous, but loss of contact is incomplete.
- The term is often used to describe the early stages in a condition which may proceed to complete dislocation.
Types of dislocations
- According to the severity: If incomplete it is called subluxation and if complete it is called dislocation.
- According to Anatomy: Anterior, posterior, superior, inferior, central or combination likes anteroinferior etc.
- According to co-existing conditions: If it is associated with fracture it is called fracture dislocation.
Treatment of dislocations
- As it obvious the mainstay of treating dislocation remains reduction of the dislocation and maintaining the same by either strapping, plaster casts, splints etc. until the surrounding soft tissues like capsules and ligaments have healed.
- Reduction must be checked radio logically immediately after reduction and from time to time as needed.
- A very important point is to achieve a congruous reduction.
PAGET’S DISEASE
- Paget’s disease is a chronic condition of bone characterized by disorder of the normal bone remodeling process.
- Characterized by excessive breakdown of bone tissue followed by abnormal bone formation.
- Also known as Osteitis Deformans is a bone disease unknown cause.
- Affecting men twice as frequently as women.
- Named after the England Surgeons Sir James Paget.
- You’ve probably heard of Paget’s disease, but you may not realize it’s the second most common metabolic bone disease, after osteoporosis. In this chronic and progressive bone-remodeling condition, large and abnormal osteoclasts increase bone resorption (breakdown) at single or multiple bone sites.
- At first, bone resorption exceeds bone formation. Eventually, normal bone-forming cells (osteoblasts) are stimulated to form new bone rapidly in a disorganized, dysfunctional way. Bones affected by Paget’s disease are larger and weaker than normal, with increased metabolism and blood supply, which in turn can lead to bone pain, arthritis, skeletal deformities, and fractures. Although the disease can affect any bone, the most common sites are the spine, skull, pelvis, and weight-bearing leg bones. Long-term observation indicates that the disease doesn’t spread from one bone to another.
Etiology
- The cause of Paget’s disease is unknown
- Disease may be caused by a virus: Paramyxo virus
- Resulting in localized abnormal osteoclastic activity typical of paget’s disease.
- Also, a person’s genes may predispose them to developing paget’s disease.
- Paget’s disease affects skeletal older bone of adults
- There is also an extremely rare form of paget’s disease in children, referred to as Juvenile Paget’s disease
- In two of every three cases of Paget’s disease, more than one bone is affected
Pathology
- Increased number of osteoclasts. Osteoclasts also often larger. The osteoblasts are normal, but are often over active, due to increased factors released by osteoclasts.
- Essentially, an accelerated rate of bone turnover – with subsequent rapid new bone formation – and this new bone does not have a normal bone matrix – the matrix is disorganised
- The bones increase in size, but become more brittle, and thus more prone to fracture.
Manifestations – Symptoms
- Paget’s disease is more commonly asymptomatic, but may exhibit a variety of non-specific symptoms due to increased bone turnover.
- The bones that are move commonly affected include the pelvis, spine, skull, and the long bone.
- Individuals may experience any or a combination of the following symptoms;
- Bone pain
- fractures
- Pain
- Stiffness
- Difficulty moving your affected joints
- Nerve damage
- Loss of balance
- bone fractures
Other symptoms …
- Hearing loss, Headaches, Osteoarthritis, visual abnormalities, Cardiac abnormalities, Skeletal Deformities
Significant Lab Tests
- Blood chemistry (blood patient who have paget’s disease) results indicate very high alkaline phosphates levels with normal serum calcium and phosphorus.
- Pagetic bone has a characteristic appearance on X-rays.
- ↑level of alkaline phosphatase in the blood.
- Normal calcium, phosphate, & aminotransferase.
- ↑- Markers of bone turnover in urine eg. Deo-pyridinoline
- ↑ – Levels of serum & urinary hydroxyproline.
- Bone scans are useful for extent and activity of the condition.
Imaging Consideration
- X-ray of the skull, spine, pelvis and long bone.
- CT scan
- MRI (Magnetic Resonance Imaging)
- Radionuclide bone scan or RNI (Radionuclide Imaging).
Radiological Appearance
- Radionuclide bone scans readily detect Paget’s disease even in its very early stage.
- Radio graphically of the affected bone typically demonstrate cortical thickening, with a coarse, thickened trabecular pattern.
Complications
- Complications of Paget disease include the following:
- Fractures (abnormal bone)
- Osteogenic Sarcoma
- Neuromuscular syndromes (compression)
- Joint disease (degenerative)
- Cardiovascular abnormalities (hyper-dynamic circulation)
Medical Management
- There is no known cure for this disease.
- Most cases are mild and asymptomatic no treatment is necessary in symptomatic cases medications.
- Bisphosphonates are required to reduce the osteoclastic activity.
- Calcium + Vitamin D + sun shine and Exercies.
- The osteoclastic/osteoblastic activity can be monitored by regular check up of serum/urinary calcium, bone specific alkaline phosphatases.
- Needs management of cardiac problems due to hyper dynamic circulation.
- Watch for Osteogenic sarcomas.
Surgical management
- Deformities may be corrected by surgical intervention (osteotomy). ORIF Open Reduction Internal Fixation may be necessary for fractures.
- Total hip or knee replacement is usually required when client with Paget’s disease develops degenerative arthritis of hip or knee May require surgery for spinal stenosis, nerve root compression
Diet and Exercise
- 1000-1500 mg of Calcium
- Adequate Sunshine
- At least 400 units of Vitamin D DAILY
Teaching Plan
- Patients over the age of 40 can be at risk for Paget’s disease.
- Medical treatment may not cure current health problems associated with Paget’s disease
- Surgery may be needed to reduce pain and increase activity.
- When taking oral medications, patients should drink 6-8 oz of water.
- Patients should remain in an upright position 30 minutes following taking medications.
- Patient should also refrain from eating for 30 minutes following oral medication
- Patients may experience heartburn with oral medications.
- Although the condition is a chronic illness, Paget’s disease focuses on the bones associated with the spine, pelvic, hip, thighs, head and arms but does not spread to new bone.
- Patient needs to adhere to frequent, regular check-ups with treating physicians
- Paget’s disease does not majorly impact the quality of patient life. Research shows many have no critical complaints while living with Paget’s disease.
TUBERCULOSIS OF BONE
- Tuberculosis affects primarily the lungs and gastrointestinal tract, but may also infect the musculoskeletal system.
Pathology
- Hematogenous dissemination to long bones and vertebrae
- Direct spread to bone from adjacent tuberculous lymphadenitis
- Single or multi centric, particularly in AIDS
- Predilection for synovium – higher oxygen pressure
- There is caseating granulomatous inflammation with bone necrosis, resulting in the destruction of bone.
- Extension of the TB osteomyelitis into joint spaces results in tuberculous arthritis. The infection crosses to the bone on the other side of the joint.
Incidence
- 3% of tuberculosis is musculoskeletal. Of these, the commonest area affected is the spine.
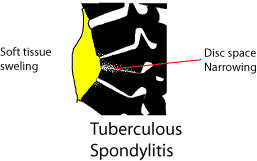
Radiological signs
- Lytic process.
- Affects both sides of a joint or disc space.
- Soft tissue swelling
- Effusion in a joint
- Paravertebral swelling in thorax
- Fusiform paravertebral swelling in the neck
- Cystic tuberculosis – causes cystic lesions in bones
- Sclerosis is a sign of healing TB – successfully treated lesions become sclerotic as they heal.
Special Investigations
- The ESR is raised often to above 100 mm/hr. On the differential white cell count there is a lymphocytosis. Sputum is taken for culture and a 24 hour urine collection can be taken if renal tuberculosis is a suspected cause.
- Serological tests such as the Mantoux or Tine test are positive. In a third world population, such as South Africa there is anyway a high incidence of positivity with these tests. A positive test merely indicates that a patient has had exposure to TB in the past. A negative test may be of more value in excluding TB, but other immunosuppressive diseases such as HIV may suppress the reaction.
Biopsy
- Biopsy may be needed is the diagnosis is in doubt. In South Africa, where tuberculosis is common, biopsy is not always done. If the blood and radiological criteria point to Tuberculosis therapy is started without a biopsy
Treatment
- Anti tuberculous drugs are started.
- (South African Medicines Formulary, fifth edition pg. 277)
Antituberculosis Drugs for Adults
| Intensive phase (2 –3 months): | Body weight <50kg | >50kg |
| Rifampisin 120mg +
Isoniasid (INH) 60 mg + Pirasinamide (PZA) 300mg + Etambutol 200mg Combination tablet (Rifafour®, Myrin Plus®) daily, 5 days per week |
4 tablets daily | 5 tablets daily |
| Maintenance phase: | <50kg | >50kg |
| Rifampisin 150mg + INH 100mg
Rifampisin 300mg + INH 150mg |
3 tablets daily
– |
-2 tablets daily |
- Pyridoxine (Vitamin B6) 10mg /day must be added in patients with inadequate intake, or at risk of developing peripheral neuropathy (pregnancy, diabetics, HIV infected patients)
- Therapy lasts at least 1 year to 18 months. The ESR should show a decrease and the lesion on X rays becomes more sclerotic.
- Failure to respond may be due to:-
- Failure to take the drugs
- Wrong diagnosis
- Drug resistant tuberculosis
Side effects of anti tuberculous drugs
| Serious: | Drug causing | Action |
| Jaundice (hepatitis) | INH, Rifampisin, PZA | Stop TB Drugs. Contact an infection specialist. |
| Skin rash with pyrexia | INH, Rifampisin | |
| Bleeding tenancy, shock, renal failure. | Rifampisin | |
| Impaired vision and color perception | Etambutol |
Splinting of joints
- The affected joint must be immobiliased in a position of function. For the hip in the acute phase it means skin traction. Once discharged from hospital the patient with hip TB is told to sleep prone to avoid a flexion contracture. The spine will need an appropriate brace. For other joints a plaster cast, back slab or a custom made splint may be necessary
Place of Surgery
- Surgery plays a limited role in the treatment of tuberculosis. Synovial biopsy may be needed to make the diagnosis. In spinal tuberculosis, gross instability or neurological fallout are indications for an anterior fusion and decompression.
- Late surgery may be needed to repair the damage by a joint being destroyed or left in an unacceptable position. Arthrodesis is sometimes the only solution in these severe cases.
 Spinal Tuberculosis
Spinal Tuberculosis
- In the thoracic spine the patient presents with a gibbus.
- There may be neurological fallout due to:
- Mechanical pressure on the spinal cord
- Vascular – blood supply to cord compromised
- TB granuloma pressing on cord
Radiology
- There is loss of disc space, soft tissue swelling is commonly seen adjacent to the involved area, or the pus may track into the
 psoas sheath (involvement about thoraco-lumbar junction)
psoas sheath (involvement about thoraco-lumbar junction) - Treatment principles remain the same as with TB of other areas. Antituberculosis medication is begun once the diagnosis is confirmed. Further deformity is prevented with a hard brace such as a Thoraco sacro lumbar orthosis (for Thoraco-lumbar involvement).
- An indication for operation is neurological compromise, unresponsive to treatment. As TB spine involves mainly the vertebral body, an anterior approach is needed. The caseous material is curetted out and the vertebral bodies fused with an anterior bone graft. The rib removed for the thoracotomy can be used for this.
BONE TUMORS
- Bone cancer, also known as primary bone cancer, is a form of cancer that develops in hard bone tissues and sometimes in the cartilage tissues of the bone. Primary bone cancer is rare, and differs from cancers that develop in: 1). other organs of the body and spread to the bones when metastasis (spreads), or 2). bone marrow cells (such as leukemia, multiplemyeloma, and lymphoma).
- Neoplasms of the musculoskeletal system are of various types, including osteogenic, chondrogenic, fibrogenic, muscle (rhabdomyogenic), and marrow (reticulum) cell tumors as well as nerve, vascular, and fatty cell tumors. They may be primary tumors or metastatic tumors from primary cancers elsewhere in the body (eg, breast, lung, prostate, kidney). Metastatic bone tumors are more common than primary bone tumors.
- Tumors may be benign (not cancer), or malignant (cancer). Also called neoplasm. Cancer is a term for diseases in which abnormal cells divide without control and can invade nearby tissues. Cancer cells can also spread to other parts of the body through the blood and lymph systems.
Types
- Bone cancer is divided into separate types based on the type of cell where the cancer started. The most common type of bone cancer include:
Osteosarcoma. Osteosarcoma begins on bone cells. Osteosarcoma occurs most often in children and young adults.
Chondrosarcoma. Chondrosarcoma begins in the cartilage cells are normally found in the bone ends. Chondrosarcoma most commonly affects older adults.
Ewing’s Sarcoma. It is not clear where ewing sarcoma begins. Ewing’s sarcoma is believed that to begin in nerve tissue in the bone. Ewing’s sarcoma occurs most often in children and young adults.
Benign Bone Tumors
- Benign bone tumors are slow growing, well circumscribed, and encapsulated. They produce few symptoms and do not cause death. Benign primary neoplasms of the musculoskeletal system include osteochondroma, enchondroma, bone cyst (eg, aneurysmal bone cyst), osteoid osteoma, rhabdomyoma, and fibroma. Benign tumors of the bone and soft tissue are more common than malignant primary bone tumors.
- Osteochondroma, the most common benign bone tumor, may become malignant. Enchondroma is a common tumor of the hyaline cartilage of the hand, femur, tibia, or humerus. Osteoid osteoma is a painful tumor that occurs in children and young adults. Osteoclastomas (giant cell tumors) are benign for long periods but may invade local tissue and cause destruction. These tumors may undergo malignant transformation and metastasize. Bone cysts are expanding lesions within the bone (eg, aneurysmal and unicameral).
Malignant Bone Tumors
- Primary malignant musculoskeletal tumors are relatively rare and arise from connective and supportive tissue cells (sarcomas) or bone marrow elements (myelomas). Malignant primary musculoskeletal tumors include osteosarcoma, chondrosarcoma, Ewing’s sarcoma, and fibrosarcoma. Soft tissue sarcomas include liposarcoma, fibrosarcoma, and rhabdomyosarcoma. Metastasis to the lungs is common. Osteogenic sarcoma (osteosarcoma) is the most common and is often fatal owing to metastasis to the lungs. It is seen most frequently in children, adolescents, and young adults (in bones that grow rapidly); in older people with Paget’s disease of the bone; and in persons with a prior history of radiation exposure. Common sites are distal femur, the proximal tibia, and the proximal humerus.
- Chondrosarcoma, the second most common primary malignant bone tumor, is a large, bulky tumor that may grow and metastasize slowly or very fast, depending upon the characteristics of the tumor cells involved. Tumor sites may include pelvis, femur, humerus, spine, scapula, and tibia. Tumors may recur after treatment.
Metastatic Bone Disease
- Metastatic bone disease (secondary bone tumors) is more common than any primary malignant bone tumor. The most common primary sites of tumors that metastasize to bone are the kidney, prostate, lung, breast, ovary, and thyroid. Metastatic tumors most frequently attack the skull, spine, pelvis, femur, and humerus and often involve more than one bone.
Stages of Bone Cancer
- Stage I: In this stage, the cancer is confined to the bone and hasn’t metastasized to other parts of the body. This stage is considered not aggressive and low grade.
- Stage II: In this stage, the cancer is confined to the bone and hasn’t metastasized to other parts of the body; however, biopsy testing reveals that the bone cancer is aggressive and high grade.
- Stage III: In this stage, the cancer is present in two or more different parts of the same bone. Biopsy testing reveals that the cancer can be either low grade or high grade.
- Stage IV: In this stage, the cancer has metastasized from the bone to other regions of the body, such as liver, lungs or brain.
Causes of Bone Cancer
- The cause of many bone cancers is not clear. Doctors believe the cancer occurs due to an error in the DNA of a cell. This error causes the cell to grow and divide uncontrollably resulting in cancer. These abnormal cells continue to live instead of dying at a particular time. The buildup of these mutated cells result in a tumor/mass, which in turn infiltrates the nearby structures and/or metastasize to other parts of the body.
Risk Factors of Bone Cancer
- Inherited genetic syndromes, such as hereditary retinoblastoma and Li-Fraumeni syndrome may cause or increase the risk of having bone cancer.
- Precancerous conditions such as Paget’s disease of bone affects the older adults and also increases the risk of developing bone cancer.
- Exposure to radiation from cancer treatment increases the risk of having a bone cancer in the future.
Symptoms of Bone Cancer
- Characteristic feature of bone cancer or bone cancer symptoms include:
Bone pain. - Swelling and pain near the affected area.
- Fracture.
- Fatigue.
- Weight loss is not desired.
- Spinal metastasis results in cord compression and neurologic deficits (eg, progressive pain, weakness, gait abnormality, paresthesia, paraplegia, urinary retention, loss of bowel or bladder control).
Assessment and Diagnostic Findings
- May be diagnosed incidentally after pathologic fracture
- CT scan, bone scan, myelography, MRI, arteriography, x-ray studies
- Biochemical assays of the blood and urine (alkaline phosphatase levels are frequently elevated with osteogenic sarcoma; serum acid phosphatase levels are elevated with metastatic carcinoma of the prostate; hypercalcemia is present with breast, lung, and kidney cancer bone metastases)
- Surgical biopsy for histologic identification; staging based on tumor size, grade, location, and metastasis
Medical Management
- The goal of treatment is to destroy or remove the tumor. This may be accomplished by surgical excision (ranging from local excision to amputation and disarticulation), radiation, or chemotherapy.
- Limb-sparing (salvage) procedures are used to remove the tumor and adjacent tissue; surgical removal of the tumor may, however, require amputation of the affected extremity.
- Chemotherapy is started before and continued after surgery in an effort to eradicate micrometastatic lesions.
- Soft tissue sarcomas are treated with radiation, limb-sparing excision, and adjuvant chemotherapy.
- Metastatic bone cancer treatment is palliative; therapeutic goal is to relieve pain and discomfort as much as possible while promoting quality of life.
- Internal fixation of pathologic fractures, arthroplasty, or methylmethacrylate (bone cement) minimizes associated disability and pain in metastatic disease.
Nursing Interventions for Bone Cancer
- Pain management
- Psychological pain management techniques (deep breath relaxation techniques, visualization, and guided imagery) and pharmacological (providing analgesic).
- Teach effective coping mechanisms
- Motivation clients and families to express their feelings, and give moral support and encourage families to consult a psychologist or clergy.
- Provide adequate nutrition
- Decreased appetite, nausea, vomiting often occur as a side effect of chemotherapy and radiation, so it should be given adequate nutrition. Antiemetic and relaxation techniques can reduce gastrointestinal reactions. Parenteral nutrition can be carried out in accordance with the indications of the doctor.
- Health education
- Patients and families are given health education on the likelihood of complications, treatment programs, and wound care techniques at home .
- If necessary; traction, Traction Treatment Principles
- Provide comfort measures (eg frequently change position, back massage) and therapeutic activity.
- Give the drug as an indication of examples; analgesic muscle relaxant.
- Give local heating as indicated.
- Give strength in early bandage / replacement in accordance with the indications, use aseptic technique correctly.
- Keep linen remains dry, free of wrinkles.
- Encourage the client to use loose cotton clothing.
- Encourage the client to use stress management, for example: guided imagery, deep breathing.
- Assess the degree of immobilization produced.
- Identification signs or symptoms that require medical evaluation, eg edema, erythema.